Causality Analysis for Public and Private Expenditures on Health Using Panel Granger-Causality Test
Su-Dong Lee, 이정혜, Chi-Hyuck Jun (2015) · industrial-engineering-and-management-systems 14(1):104-110 · DOI ↗
공공 vs 민간 의료 지출 사이의 crowding-out 가설 — “공공 의료 지출 증가가 민간 의료 지출을 감소시키는가” — 을 OECD 17 개국 (1980-2010) 패널에 panel-granger-causality-test (Holtz-Eakin-Newey-Rosen 1988) 로 검정. 핵심 발견: 미국 제외 16 개국에서 공공 의료 지출 이 3-4 년 시차를 두고 민간 의료 지출 에 유의한 음의 효과 (, , ). 미국은 outlier — 절대 규모 + 공공/민간 비율 모두 다른 국가와 distinctive. SIC 기반 lag 11 선택, Levin-Lin-Chu 단위근 검정 후 1차 차분. 이정혜 의 POSTECH 박사 시기 의 방법론적 확장 + 정책 응용 첫 접촉. Crowding-out 가설의 첫 OECD 패널 정량 검정.
- RQ: 한 국가의 공공 의료 지출 (PUB) 증가가 민간 의료 지출 (PRIV) 을 감소시키는가? — 광범위 crowding-out 가설의 정량 검정. 어느 시차에서? 모든 국가에서 일관된가?
- 방법론: panel-granger-causality-test (Holtz-Eakin-Newey-Rosen 1988 의 panel VAR), levin-lin-chu-unit-root-test (Levin-Lin-Chu 2002, 단위근 검정), holtz-eakin-newey-rosen-panel-var (country fixed effect + lag VAR), SIC (Schwarz Information Criterion) 의 optimal lag length 선택, leave-one-out robustness test, 패널 데이터 분석. EViews 7 사용
- 데이터: OECD Health Database (2013.6 버전), 17 개국 (Australia, Austria, Canada, Denmark, Finland, Germany, Iceland, Ireland, Japan, Korea, New Zealand, Norway, Portugal, Spain, Sweden, UK, US) × 31 년 (1980-2010), 인당 PUB + PRIV 의료 지출. De-inflation (inflation rate 제거) → 1차 차분 ()
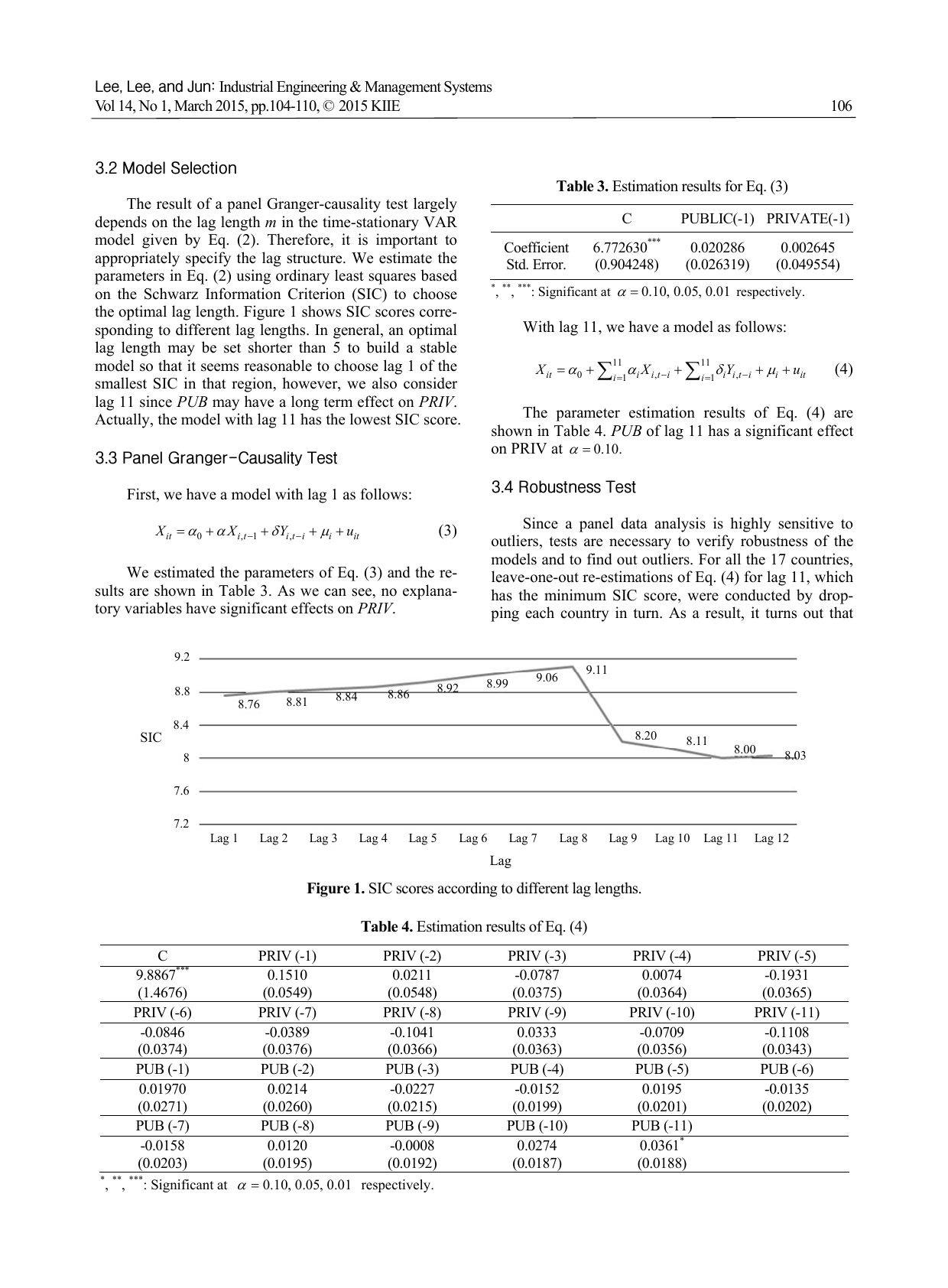
- 주요 발견: (i) Lag 1 모형 무의미 — 즉시 효과 없음 (Table 3, PUB(-1) coef = 0.020, n.s.). (ii) Optimal lag = 11 (SIC 최소화) — long-term effect 의 우선 가설. Table 4 의 17 국 estimation: PUB(-11) 만 유의 (, ) 이고 부호는 양 — 가설과 반대 방향. (iii) Leave-one-out robustness — US 제외 시 full pattern 반전 (Table 5a): PUB(-3) = −0.032* + PUB(-4) = −0.030* 이 유의한 음의 효과. US 의 outlier 영향. (iv) 16 개국 (US 제외) 의 최종 모형 (Table 6): PUB(-3), PUB(-4) 가 유의 (음). PRIV 도 lag 1, 3, 5, 6, 8, 10, 11 에서 자기상관. (v) Cross-national robustness (Appendix): 15 개국 (Austria 도 제외) 의 leave-one-out 에서 PUB(-3), PUB(-5) 의 음 효과 유지 — systematic
- 시사점: (a) 3-4 년 시차의 crowding-out 정량 확인 — 의료 정책의 효과 evaluation horizon 은 3-4 년 후 가 적절. (b) US 의 exceptional 위치 — 의료 시장 구조 (Medicare/Medicaid + 민간 보험 dominance) 가 다른 OECD 와 근본적으로 다른 dynamic. (c) Public-Private 부문 상호의존성 — 단일 부문 분석 (공공만 또는 민간만) 의 systematic bias. (d) 공공 의료 보장 확대의 부분적 substitution — full crowding-out 아니지만 marginal 효과. (e) 후속 연구: PUB·PRIV 의 asymmetric lag + macroeconomic variable (GDP, inflation) + 건강 결과 (smoking, obesity) 추가
요약
이 paper 는 이정혜 의 POSTECH Industrial & Management Engineering 박사 시기 (1 기) 의 방법론적 확장 + 정책 분석 첫 접촉 작업. Su-Dong Lee 제 1 저자 + Chi-Hyuck Jun (지도교수, corresponding author) 의 POSTECH 공저. 동기는 정책 가설의 정량 검증 부재 — 정책 입안자들이 공공 의료 지출 증가가 민간을 감소시킨다 는 substitution / crowding-out 가설을 widely held belief 로 가정하지만, 실증 연구가 없다. Tuohy et al (2004) 가 반대 방향 (민간 → 공공 효과) 만 검정. Akinkugbe-Afeikhena (2006), Anyanwu-Erhijakporn (2007) 등은 의료 지출 → 건강 outcome 의 효과 (consensus 없음). 본 paper 는 PUB ⇄ PRIV 의 양방향 Granger 인과를 OECD 17 개국 1980-2010 패널에서 검정.
방법론은 3 단계. Stage 1 — 단위근 검정. levin-lin-chu-unit-root-test (Levin-Lin-Chu 2002) 로 PUB · PRIV 의 stationarity 검정. Level 에서 단위근 존재 (PUB stat = 6.50, = 1.000; PRIV stat = 3.51, = 0.999, 비기각). 1차 차분 후 단위근 기각 (PUB stat = −8.97, < 0.001; PRIV stat = −8.08, < 0.001) → stationary. Stage 2 — Lag 선택. Schwarz Information Criterion 의 1-22 lag 비교. Lag 1 의 first local minimum 후 lag 11 의 global minimum — short-term 과 long-term 두 가설 동시 검정. Stage 3 — Panel VAR estimation. Holtz-Eakin-Newey-Rosen (1988) 의 country-fixed-effect + lag VAR. Lag 1 모형 (Table 3): PUB(-1) coef = 0.020, n.s. — 즉시 효과 없음. Lag 11 모형 (Table 4): PUB(-11) 만 유의 () — 양의 효과는 crowding-out 가설과 반대.
Stage 4 — Robustness. Leave-one-out cross-national stability test. 17 국 중 1 국씩 제외해 16 국 패널로 재추정. 4 개국 (Ireland, Norway, Japan, US) 제외 시 PUB(-11) 의 유의성 소실. US 제외가 결과를 가장 크게 변화 — 모든 lag 의 부호 + 유의성 패턴 반전. US 제외 16 국 (Table 5a, Table 6): PUB(-3) = −0.032* + PUB(-4) = −0.030* + PRIV(-4) = +0.098* 의 유의. 공공 의료 지출 → 3-4 년 시차 → 민간 의료 지출 음의 효과 가 US 제외 OECD 의 일관된 패턴. Figure 2 비교: US 의 PUB + PRIV 절대 규모 + PUB/PRIV 비율 이 다른 16 개국과 distinct — Medicare/Medicaid + 민간 보험 시장 구조 가 OECD 표준에서 systematic deviation. 결론: (i) US 제외 16 개국에서 3-4 년 시차 crowding-out 정량 확인, (ii) US 는 별도 case study 필요, (iii) 정책 evaluation horizon 은 3-4 년 후 가 적절. 한계: (i) 단일 dependent variable (PRIV) 의 unidirectional 검정 — PRIV → PUB 역방향 검정 미수행, (ii) lag 11 의 over-parameterization 가능, (iii) macro covariate (GDP, demographic) 미통제, (iv) sub-period (예: 1980s vs 2000s) heterogeneity 미검정.
핵심 결과
Levin-Lin-Chu 단위근 검정 (17 OECD, 1980-2010)
| 변수 | Level Stat | 1차 차분 Stat | ||
|---|---|---|---|---|
| PUBLIC (PUB) | 6.4972 | 1.0000 | −8.9743 | 0.0000 |
| PRIVATE (PRIV) | 3.5081 | 0.9998 | −8.0846 | 0.0000 |
→ Level non-stationary, 1차 차분 stationary.
Lag 1 모형 (Table 3, 17 국)
| C | PUB(-1) | PRIV(-1) | |
|---|---|---|---|
| Coef | 6.773*** | 0.020 | 0.003 |
| SE | (0.904) | (0.026) | (0.050) |
→ 즉시 효과 없음.
Lag 11 모형 — US 제외 16 국 (Table 6, 핵심 발췌)
| 변수 | Coef | SE |
|---|---|---|
| C | 6.139*** | 1.208 |
| PUB(-3) | −0.032* | 0.019 |
| PUB(-4) | −0.030* | 0.018 |
| PUB(-1) | 0.014 | 0.024 |
| PUB(-11) | 0.023 | 0.017 |
| PRIV(-4) | 0.098* | 0.052 |
| PRIV(-5) | −0.052 | 0.054 |
*<0.10, **<0.05, ***<0.01.
정량 결론. PUB → PRIV 의 음의 인과 (crowding-out) 가 3-4 년 시차에서 유의 (, , 모두 ). US 의 outlier 영향 — US 포함 17 국 모형에서는 이 효과 가려짐. 의료 정책 효과 evaluation 의 적정 horizon 이 3-4 년임을 시사.
방법론 노트
panel-granger-causality-test (Holtz-Eakin-Newey-Rosen 1988):
여기서 = country year 의 PRIV (1 차 차분), = PUB (1 차 차분), = country-specific fixed effect (시간 불변 idiosyncratic 특성), = 평균 0, country independent disturbance, = lag 길이.
Granger causality 가설:
기각 시 PUB Granger-causes PRIV. Joint F-test 또는 individual coefficient -test.
Lag 선택은 SIC (Schwarz Information Criterion):
여기서 = residual variance, = sample size. SIC minimize 의 lag = optimal.
식별은 (i) 17 국 × 31 년 = 527 obs (lag 11 후 effective 17 × 20 = 340 obs), (ii) country fixed effect 가 time-invariant heterogeneity 통제 (예: 의료 시스템 design 차이), (iii) 1 차 차분 후 stationary 가정의 Levin-Lin-Chu test 확인, (iv) leave-one-out 의 cross-national stability check. Limitation: (a) PUB ↔ PRIV의 simultaneity 미통제 (Holtz-Eakin GMM 의 strict exogeneity 가정), (b) macro covariate (GDP, 인구 고령화) 미통제, (c) 단일 lag length (PUB · PRIV 동일 ) 의 over-restriction.
연구 계보
본 paper 의 Granger-causality lineage: Granger (1969 Econometrica) 의 causality definition — predictive error variance reduction 으로 인과 정의. Panel Granger 라인: Holtz-Eakin-Newey-Rosen (1988 Econometrica) 의 panel VAR + country fixed effect; Levin-Lin-Chu (2002 Journal of Econometrics) 의 panel unit root. 건강-경제 응용 라인: Hartwig (2010 Journal of Macroeconomics) 의 health capital → long-term growth panel Granger, Motonishi-Yoshikawa (1999 JJIE) 의 Japan financial vs real causes panel Granger. Public-Private 의료 가설 라인: Tuohy-Flood-Stabile (2004 Journal of Health Politics, Policy and Law) 의 민간 financing → 공공 의료 시스템 효과 (반대 방향). 건강 지출 → 건강 outcome 라인: Akinkugbe-Afeikhena (2006), Anyanwu-Erhijakporn (2007), Musgrove (1996), Burnside-Dollar (1998) — 합의 없음.
TEMEP 내 sibling: 본 paper 는 이정혜 의 POSTECH 박사 시기 (1 기, 2010-2014) 의 정책 분석 분기 의 씨앗 — 주류 라인은 MB 특성 선택 (chemometrics), 본 paper 는 시계열 인과 + 의료 정책 의 첫 응용. junghyelee-2018-monte-carlo-mb-multivariate-calibration 의 chemometrics 라인 과는 다른 주제적 분기 — 두 라인이 3 기 SNU TEMEP 시기에 medical AI + 기술 정책 분석 으로 통합 (예: Risk score-embedded deep learning for biological age estimation: Development and validation, TMF-GNN: Temporal matrix factorization-based graph neural network for multivariate time series forecasting with missing values). 이정혜 author page 의 방법론적 다양화 + 정책 응용 anchor. Chi-Hyuck Jun 은 이정혜 의 박사 지도교수 — POSTECH IME 의 Industrial & Management Engineering 시각의 의료 데이터 분석 라인. 본 paper 는 이정혜 가 TEMEP 부임 후 의 기술경영 + 의료 응용 방향 전환의 intellectual seed.
See also
- panel-granger-causality-test
- levin-lin-chu-unit-root-test
- holtz-eakin-newey-rosen-panel-var
- 패널 데이터 분석
- public-health-expenditure
- private-health-expenditure
- Crowding-out 효과
- oecd-health-data
- 이정혜
- Su-Dong Lee
- Chi-Hyuck Jun
- Risk score-embedded deep learning for biological age estimation: Development and validation
- industrial-engineering-and-management-systems
인접 그래프
- 인물 3
- 방법론 1
- 주제 1
- 논문 2