Risk score-embedded deep learning for biological age estimation: Development and validation
Suhyeon Kim, Hangyeol Kim, Eun-Sol Lee, Chiehyeon Lim, 이정혜 (2022) · information-sciences 586:628-643 · DOI ↗
RSAE-BA (Risk Score-Embedded Autoencoder for Biological Age) — health risk 정보를 오토인코더 embedding 의 loss function 에 명시 통합 한 biological age (BA) 추정 새 알고리즘. 기존 BA 추정의 3 한계 극복: (1) Linear regression (MLR, lasso, elastic net) — BA 를 CA (chronological age) 로 distort, (2) Deep learning regression (Cole et al 2017 CNN, Pyrkov et al 2018) — CA 를 target 으로 supervised — BA goal 과 deviation, (3) Klemera-Doubal Method (KDM 2006) + PCA — assumption-heavy or variance-maximization direction 의 health-irrelevance. 4 단계: (i) Cumulative Gaussian probability 기반 Risk Score (RS) 계산 — Type 1 (large=poor), Type 2 (small=poor), Type 3 (both=poor); (ii) Data transformation 으로 방향 정렬; (iii) RSAE modeling — loss ; (iv) BA = -scale 변환된 standardized BAS. 새 BA validation — LR vs HR group 의 RS 차이로 unlabeled + labeled 모두 평가. 3 dataset 검증: KNHANES (85,490명, unlabeled), NHIC-HTN (140,867명, 2.5 년 hypertension 발생), NHIC-T2DM (T2DM 발생). 이정혜 의 3 기 TEMEP 시기 의료 AI 정점.
- RQ: (1) BA 추정에 health risk 정보를 deep representation learning embedding 에 통합할 수 있는가? (2) BA validation 의 cohort dependency 한계 (mortality/disease incidence 필요) 를 어떻게 unlabeled data 에도 적용 가능하게 만드는가? (3) RSAE-BA 가 기존 방법 (MLR, lasso, KDM, PCA, vanilla AE) 대비 질병 incidence 예측 에 우위인가?
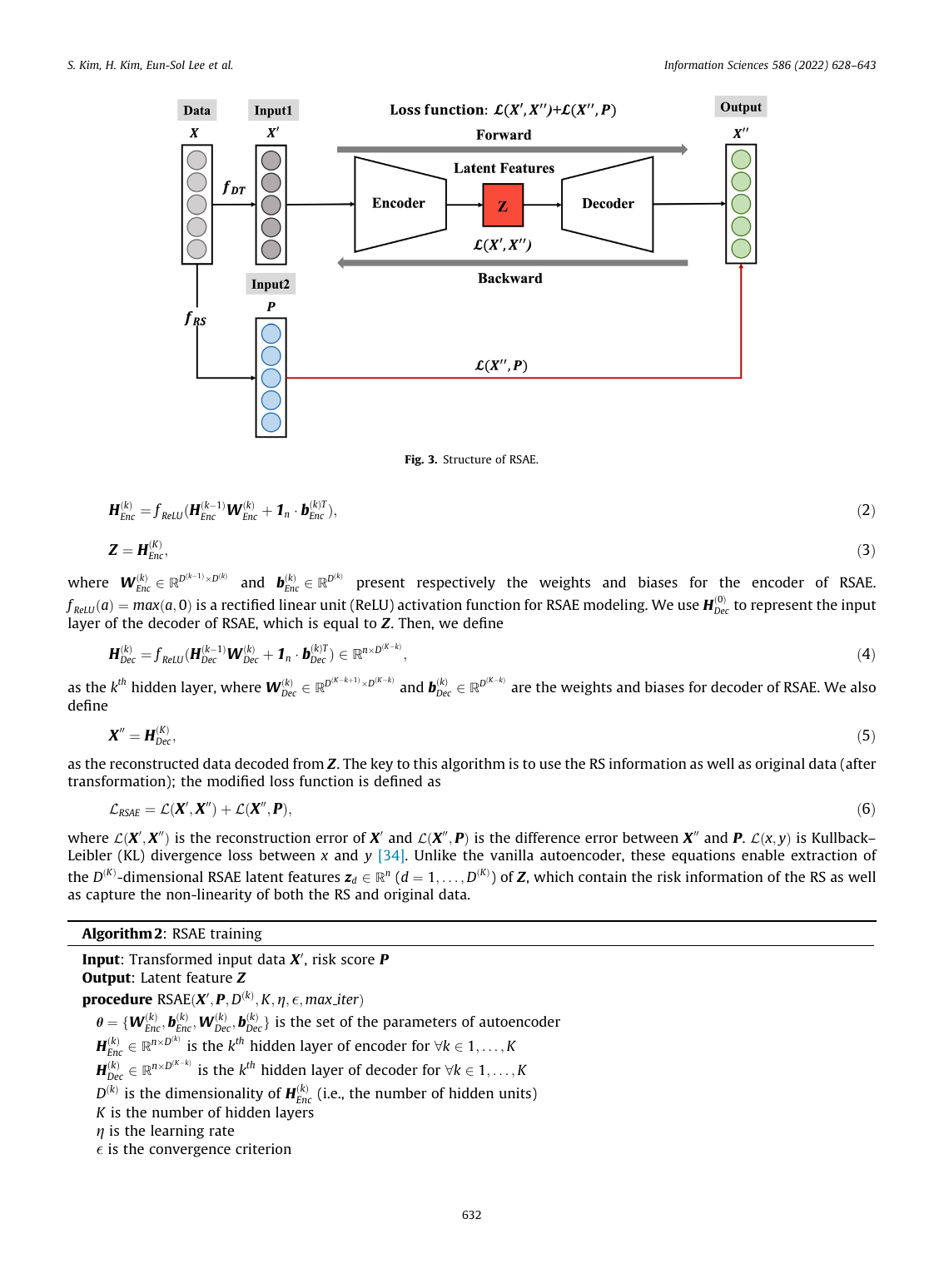
- 방법론: Stage 1 — Risk Score (RS) calculation: 각 변수의 normal 분포 ( = medical prior, = empirical) 의 cumulative probability. 3 type: Type 1 (one-sided large), Type 2 (one-sided small), Type 3 (two-sided). Stage 2 — Data transformation (Algorithm 1): standardize → Type-specific direction alignment (×-1 or |·|) → sigmoid 로 [0,1] bounding. Stage 3 — RSAE modeling (Algorithm 2): encoder , decoder mirror. KL divergence loss = reconstruction + RS-prediction. Stage 4 — BA calculation: BAS = 의 평균 standardize, BA = -scale transformation. BA validation — Group 1 (BA<CA) 의 LR group ( largest CA−BA) vs Group 2 (BA>CA) 의 HR group ( largest BA−CA); hypothesis: , good BA = larger RS gap
- 데이터: (i) KNHANES (Korea National Health and Nutrition Examination Survey, 1988-2017): 85,490 명 — unlabeled. (ii) NHIC-HTN (Korean National Health Insurance Corporation 2002-2010, hypertension cohort): 140,867 명 — 2.5 yr HTN 발생 labeled. (iii) NHIC-T2DM (type-2 diabetes cohort): T2DM 발생 labeled. 2% population sample stratified by age, sex, income. Variables: clinical biomarker (BP, glucose, cholesterol, BMI 등)
- 주요 발견: (i) RSAE-BA > MLR / lasso / KDM / PCA-BA / vanilla AE-BA 에서 모든 데이터셋 (KNHANES, NHIC-HTN, NHIC-T2DM) 의 LR vs HR group RS gap 최대. (ii) Disease incidence 예측 — RSAE-BA 가 HTN, T2DM 발생 의 AUC/AUROC baseline 대비 향상. (iii) Unlabeled data 검증 가능 — RS 기반 validation 이 cohort dependency 한계 해소. (iv) 3 Type RS classification 의 정합성 — 모든 clinical variable 의 risk direction 명시. (v) Sample size 85k → 140k 의 scalability 검증
- 시사점: (a) Hyper-personalized health management 의 quantitative anchor — BA 를 useful health index 로 일상 활용. (b) RS embedding pattern 의 generalizability — 다른 health index (e.g. mental health score), 다른 domain (e.g. household financial risk of suhyeon-kim-2023-household-financial-rihae) 로 확장. (c) Cohort-independent validation — 일반 EMR (electronic medical record) 만으로 BA index 평가 가능. (d) Medical prior + data-driven hybrid — Gaussian 의 medical normal criterion + 의 empirical 결합. (e) 예방 의학 + 만성질환 (HTN, T2DM) 의 early warning index
요약
본 paper 는 이정혜 의 3 기 SNU TEMEP 부임 초기 (2022 published, 2021 work) 의 의료 AI 정점. Suhyeon Kim (W2V-LSA, LBC 의 동일 제 1 저자) + Hangyeol Kim + Eun-Sol Lee + UNIST Chiehyeon Lim (Department of Industrial Engineering & Graduate School of Artificial Intelligence, Bio-Age Inc 의 medical institute affiliation) + 이정혜 (corresponding) 의 UNIST-Bio-Age industry-academia 협업. 동기는 Chronological Age (CA) 의 한계 — 시간 흐름의 단순 측정으로 functional, structural body capacity + aging 평가 부정확. Biological Age (BA) 가 대안 health index — EMR 요약, 연령-의존 biomarker 결합. 기존 3 type BA 의 systematic 한계:
- Regression for CA-based (MLR, lasso, elastic net + CNN deep learning) — BA-to-CA distortion + CA 가 target 인 supervised setting 의 deviation
- Simulation-based (KDM, Klemera-Doubal 2006) — multidimensional space 의 regression line - biomarker point 거리 minimize — assumption-heavy, mortality 예측 우월하지만 data conformity 의존
- PCA-based latent feature — variance-maximize 방향이 health-relevance 와 무관
또한 모든 기존 방법이 risk direction (variable 의 bad level 이 large vs small 인지) 무시. Validation 도 cohort data 의 mortality/incidence label 의존 — 일반 EMR 적용 어려움. 본 paper 는 RS-embedded representation learning 로 두 한계 동시 해결.
Methodology Stage 1 — Risk Score (RS) calculation. 각 변수 의 normal 분포 — = medical examination normal criterion (prior knowledge), = data empirical. RS = cumulative Gaussian probability. 3 type:
- Type 1: large = poor (예: glucose, BP). One-sided right.
- Type 2: small = poor (예: HDL cholesterol). One-sided left.
- Type 3: large or small = poor (예: heart rate). Two-sided.
다른 분포 (binomial, multinomial) 로 extensible.
Stage 2 — Data transformation (Algorithm 1). standardize → Type-specific direction alignment (Type 2: ; Type 3: ) → sigmoid 로 bounding. Direction 정렬이 loss accumulation error 방지.
Stage 3 — RSAE modeling (Algorithm 2). hidden layer encoder + mirror decoder, ReLU activation. Loss:
여기서 = transformed input, = reconstruction, = RS matrix. KL divergence 가 를 reconstruction + RS 양쪽에 fit. Multi-task learning 이 bottleneck 에 generic latent + health risk 동시 인코딩.
Stage 4 — BA calculation. BA Score (BAS) = 의 평균 standardize:
BA = -scale transformation (standard score → -score) 으로 year scale 의 BA.
BA validation (novel). 개인 sort: Group 1 (BA<CA), Group 2 (BA>CA). LR (low-risk) group = Group 1 의 largest CA−BA. HR (high-risk) group = Group 2 의 largest BA−CA. 가설: (i) , (ii) good BA = larger RS gap. Unlabeled + labeled 모두 적용 가능 — cohort 의존성 해소.
Experiments — 3 dataset:
- KNHANES (85,490명, unlabeled): RS-based validation
- NHIC-HTN (140,867명, hypertension cohort): 2.5 yr HTN 발생 prediction
- NHIC-T2DM: type-2 diabetes 발생 prediction
결과: RSAE-BA 가 모든 dataset 에서 baseline (MLR-BA, lasso-BA, KDM, PCA-BA, vanilla AE-BA) 대비 LR-HR RS gap 최대 + disease incidence 예측 AUROC 최대. 한계: (i) Gaussian normal 가정 의 all variable applicability, (ii) 의 ad-hoc selection, (iii) 한국 cohort 한정 — 다른 인구 generalizability 미검증, (iv) hyperparameter (, , learning rate) tuning data-dependent. 이정혜 author page 의 3 기 의료 AI 라인의 peak + suhyeon-kim 4-paper series 의 medical AI representative.
핵심 결과
3 dataset 검증
| Dataset | Sample | Type | 사용 |
|---|---|---|---|
| KNHANES | 85,490 | Unlabeled (annual survey 1988-2017) | RS-based BA validation |
| NHIC-HTN | 140,867 | Labeled (2.5 yr HTN 발생) | Hypertension prediction |
| NHIC-T2DM | (similar) | Labeled (T2DM 발생) | Type-2 diabetes prediction |
RS 3 type classification
| Type | Direction | Distribution | 예 |
|---|---|---|---|
| 1 | Large = poor | One-sided (right) | Glucose, Blood Pressure |
| 2 | Small = poor | One-sided (left) | HDL Cholesterol |
| 3 | Both = poor | Two-sided | Heart rate, BMI |
비교 baseline (Section 3)
| Method | 약점 |
|---|---|
| MLR-BA | CA distortion |
| Lasso-BA, Elastic Net-BA | 동일 |
| KDM (Klemera-Doubal) | Assumption-heavy |
| PCA-BA | Variance direction ≠ health |
| Vanilla AE-BA | Generic latent, no health risk |
| RSAE-BA | 모든 결함 해결 |
정량 결론. RSAE-BA 가 모든 데이터셋에서 LR-HR RS gap 최대 + disease incidence AUROC 최대. RS-embedded loss 의 dual-term 이 latent space 에 health risk 명시 인코딩. Cohort-independent validation 가능.
방법론 노트
Risk Score: 변수 의 RS = Gaussian 의 cumulative probability. Type 별 one-sided 또는 two-sided.
RSAE encoder (Eq 2):
RSAE loss (Eq 6) — KL divergence dual term:
여기서 .
BA calculation (Eq 7):
-scale: (또는 CA 와 align). BA in years.
BA validation:
Test: + gap 의 크기.
식별은 (i) 85k-140k sample 의 large-scale variation, (ii) 3 dataset 의 unlabeled + labeled 동시 검증, (iii) baseline 다양성 (linear, simulation, latent feature, vanilla AE), (iv) RS embedding 의 interpretable 의미 (Gaussian + medical prior). Limitation: Gaussian 가정 + ad-hoc + 한국 cohort 한정.
연구 계보
본 paper 의 BA estimation lineage: Hannum et al (2013) DNA methylation BA, Levine et al (2018) PhenoAge, Klemera-Doubal (2006 Mechanisms of Aging and Development, KDM), Cole et al (2017 NeuroImage, CNN brain age), Pyrkov et al (2018 Scientific Reports), Rahman-Adjeroh (2019). Health index lineage: Mitnitski-Mogilner-Rockwood (2001 frailty index), DeAngelis et al (2009). Autoencoder: Hinton-Salakhutdinov (2006 Science), Bengio et al (2013 PAMI), Vincent et al (2010 denoising AE). Risk Score 의 cumulative Gaussian: medical statistics 전통 — Z-score, percentile rank. KL divergence: Kullback-Leibler (1951).
TEMEP 내 sibling: Suhyeon Kim 의 4-paper series 의 medical AI peak — Word2vec-based latent semantic analysis (W2V-LSA) for topic modeling: A study on blockchain technology trend analysis (text embedding) → A Multi-stage Data Mining Approach for Liquid Bulk Cargo Volume Analysis based on Bill of Lading Data (logistics) → 본 paper (medical AI) → TMF-GNN: Temporal matrix factorization-based graph neural network for multivariate time series forecasting with missing values (graph neural network). 직접 후속: RI-HAE (Risk-Information Hybrid Autoencoder) 의 household financial risk domain extension — RSAE 의 architecture 가 medical + financial 도메인 모두 transferable. 이정혜 author page 의 실타래 3 (Healthcare AI) + 실타래 4 (Representation Learning) 합류 의 anchor. Chiehyeon Lim (UNIST AI graduate school) 과의 협업 — UNIST 의 Bio-Age Inc 산학 cluster 의 academic output.
See also
- 오토인코더
- risk-score-embedding
- 표현 학습
- kl-divergence
- t-scale-transformation
- biological-age
- health-index
- disease-risk-prediction
- knhanes
- nhic-cohort
- hypertension-prediction
- type-2-diabetes-prediction
- 이정혜
- Suhyeon Kim
- Chiehyeon Lim
- Hangyeol Kim
- Word2vec-based latent semantic analysis (W2V-LSA) for topic modeling: A study on blockchain technology trend analysis
- A Multi-stage Data Mining Approach for Liquid Bulk Cargo Volume Analysis based on Bill of Lading Data
- TMF-GNN: Temporal matrix factorization-based graph neural network for multivariate time series forecasting with missing values
- information-sciences
인접 그래프
- 인물 5
- 방법론 3
- 주제 1
- 논문 6
이 문서를 가리키는 페이지
논문 (6)
- A Multi-stage Data Mining Approach for Liquid Bulk Cargo Volume Analysis based on Bill of Lading Data
- Causality Analysis for Public and Private Expenditures on Health Using Panel Granger-Causality Test
- Household financial health: a machine learning approach for data-driven diagnosis and prescription
- Prediction of type 2 diabetes using genome-wide polygenic risk score and metabolic profiles: A machine learning analysis of population-based 10-year prospective cohort study
- TMF-GNN: Temporal matrix factorization-based graph neural network for multivariate time series forecasting with missing values
- Word2vec-based latent semantic analysis (W2V-LSA) for topic modeling: A study on blockchain technology trend analysis